
Flap course Day1
Omdurman teaching hospital
Upper limb & anterior trunk The lateral arm flap
Innervation: posterior cutaneous nerve of the forearm.
Blood supply: posterior radial collateral artery.
Artery: Small caliber, often less than 1.5 mm.
Vein(s): The venae are typically paired and the dominant is similar in size to the artery..
Pedicle length: Short. It does not reach proximal to the proximal edge of the flap unless the flap is designed very distally.

Marking the flap outline. The axis of the flap lies over the lateral intermuscular septum. The more distal the flap is made, the thinner the skin. It can be based very distally, as a lateral forearm flap.
The axis of the humerus is marked from the deltoid insertion to the lateral epicondyle. The lateral arm flap is designed with its longitudinal axis on this marking. The skin of the arm is pinched to judge the maximum with of the flap is a large paddle is needed. Usually, four to five centimeters are the widest a flap can be. The flap can be quite long however, from the deltoid insertion to distal to the lateral epicondyle. Alternatively, a lateral forearm flap can be marked using the distal think skin around the lateral epicondyle, as shown in the diagram.

The flap is supplied by the radial collateral artery. It originates from the brachial artery and wraps posteriorly around the humerus, descending on the lateral aspect of the humerus and then branching into an anterior and posterior segments. The posterior branch supplies the lateral arm and lateral forearm flaps.

Anatomy of the lateral arm flap. The radial nerve travels across the proximal base of the flap. It sends a sensory branch with the pedicle of the flap that supplies the distal lateral arm.


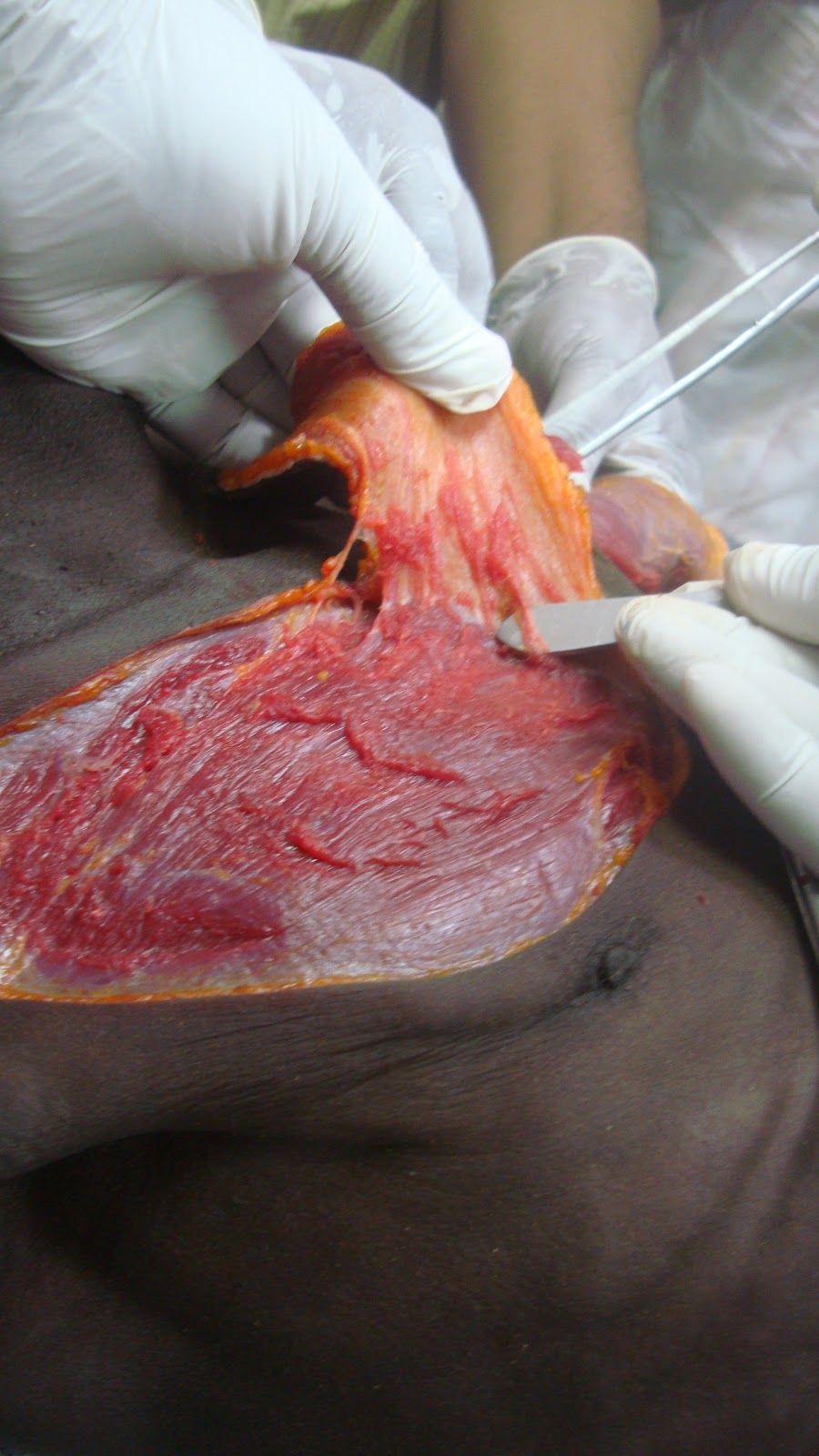
Posterior flap elevation is performed first. The flap is elevated deep to the muscular fascia. The fascial is peeled anteriorly until the septum is encountered.

The anterior aspect of the flap is then elevated until the septum, and then the flap can be raised from distal to proximal. The septal attachment to the humerus is released as the flap is elevated.
|
| The lateral arm flap has long been the workhorse of microvascular surgeons in the cover of small and moderate-sized defects, especially in the head, neck, and the extremities. Its versatility, however, has always been restricted by its small skin paddle |

The lateral Arm Osteocutaneous Flap The lateral arm flap can also be harvested as an osteocutaneous flap. The wedge of bone with periosteal cuff is harvested under the septum and septal pedicle. A narrow portion of bone approximately 1 to 1.5 centimeters wide can be harvested.






{kind=link}