
Flap course Day1
Omdurman teaching hospital
Upper limb & anterior trunkDeltopectoral flap

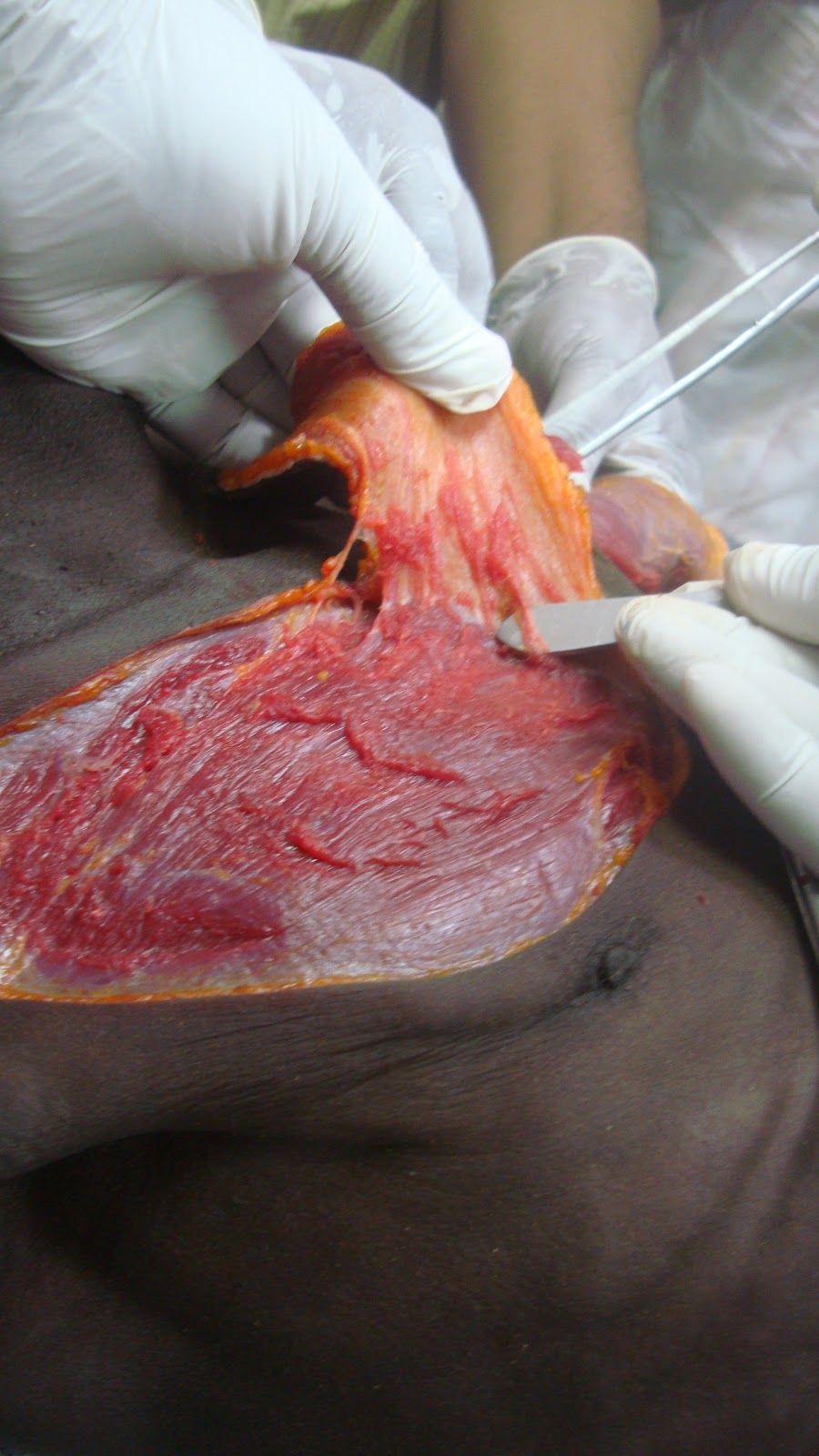
Deltopectoral Flap, was developed by Bakamjian as an axial-pattern skin flap, and its blood supply depends on perforating branches from the internal mammary artery. The main blood supply of the deltopectoral flap is provided by the second and third intercostal arteries. Deltoid portion is random.
Indications
- Carotid coverage after pharyngocutaneous fistula formation
- for cervical and neck reconstructions
- Hypopharyngeal reconstruction
- Sternum reconstructions
- Oral cavity & floor of the mouth
- Paired Deltopectoral Flap was prescribed for lower lip reconstruction.
Contraindications
- For most cases, other flaps are a better choice.
- Prior chest wall surgery or injury (eg, radical mastectomy, pacemaker)
- Prior cardiac surgery with use of internal mammary artery for bypass
Consent Inclusions
- Chest wall and neck scar
- Possible need for skin grafting to shoulder
- Bleeding, infection
- Flap failure (distal necrosis possible)



Interesting Classification of sternal wounds: Pairolero and Arnold have based their classification of sternal wounds on timing of presentation of infection; this classification divides wounds into 3 categories.This classification system does not indicate the type of reconstruction necessary for management of each type of sternal wound. Type II and III wounds are typically referred to plastic surgeons for reconstruction.
- Type I: Type I wounds occur in the first few days postoperatively, contain early wound separation with or without sternal instability, and are characterized by serosanguineous drainage without cellulitis, osteomyelitis, or costochondritis.
- Type II: Type II wounds occur within the first few weeks and are characterized by drainage, cellulitis, mediastinal suppuration, and positive cultures. Type II wounds are characterized by fulminant mediastinitis.
- Type III: Type III wounds occur months to years after surgery and are characterized by the presence of chronic draining sinus tracts, localized cellulites, osteomyelitis, or retained foreign bodies. Mediastinitis is a rare complication of type III wounds.
No comments:
Post a Comment